WATERLOO — The pandemic “opened our eyes” to existing inequalities that create greater risk for certain communities, and a Waterloo health-systems researcher is hopeful those issues will begin to be addressed once COVID-19 subsides.
“Maybe the pandemic shouldn’t just pass by us once we get vaccinated and then we’re back to normal and things get back to normal and we forget about how this affected us differently,” said the University of Waterloo’s Moses Tetui.
https://www.therecord.com/news/waterloo-region/2021/06/28/covid-19-pandemic-exposed-long-standing-inequities.html
WATERLOO — The pandemic “opened our eyes” to existing inequalities that create greater risk for certain communities, and a Waterloo health-systems researcher is hopeful those issues will begin to be addressed once COVID-19 subsides.
“Maybe the pandemic shouldn’t just pass by us once we get vaccinated and then we’re back to normal and things get back to normal and we forget about how this affected us differently,” said the University of Waterloo’s Moses Tetui.
 Are the COVID vaccine side effects the same for Black people compared to those who are not Black?
Yes, there is no evidence that the side-effects from COVID-19 vaccines are different for any ethnic or racialized group. For all the vaccines approved in Canada, most people experience a sore arm for a few days after the vaccine. Around half of people experience tiredness and a headache, and less than half have body aches, chills or feel feverish. These are all normal and expected side effects and are common with many other vaccines as well. They are signs that the immune system is learning how to recognize COVID.
For all these vaccines, these side effects will happen within a day or two of getting the vaccine and will disappear by the third or fourth day for most people. While there is a small chance that there will be a serious side effect, these are rare. Rare but serious side effects might be something like an allergic reaction. It’s always a great idea to speak with a health professional about any serious allergies or other health conditions or concerns you may have before you receive any vaccine.
Are vaccines developed with considerations given to how they might affect Black people different from other races?
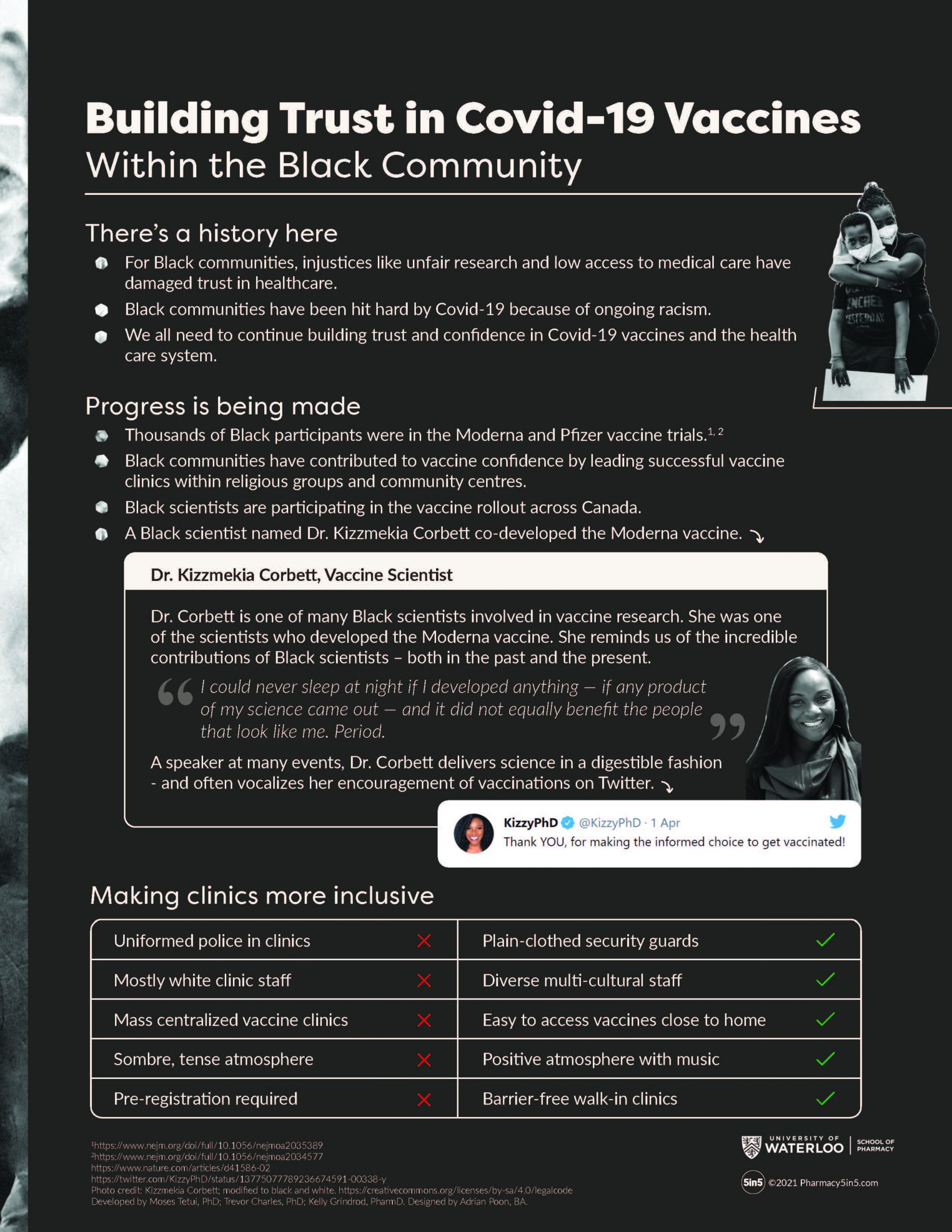
Yes, around 10 per cent of the Pfizer and Moderna trial populations identified as Black. The studies demonstrated that there were no differences in efficacy or safety in any racialized or ethnic group. It is also important to note that there is no known evidence that would suggest that vaccines affect people differently based on racial differences. In the past, Black and Indigenous communities were used to test vaccines in what has widely been criticized and categorized as unethical today. The Moderna vaccine was co-developed by a Black immunologist named Dr. Kizzmekia Corbett.
Is the wait-and-see approach adopted by some members of the Black community before receiving their first dose putting them at greater risk?
Yes, vaccination is the best protection against severe disease arising from COVID-19 infection. Systemic racism means Black communities are more likely to live in crowded housing conditions or to work in higher-risk environments. When some members of the Black community decide “to wait and see” it can further increase the risk of COVID within the community. Often, people use a “wait and see” approach when they have certain questions or concerns about the vaccines. A better approach would be to discuss those concerns with a trusted health care provider or community leader. It’s important to note that the wait and see approach could have a similar risk for any racial or ethnic group depending on their risk of exposure.
Are the COVID vaccine side effects the same for Black people compared to those who are not Black?
Yes, there is no evidence that the side-effects from COVID-19 vaccines are different for any ethnic or racialized group. For all the vaccines approved in Canada, most people experience a sore arm for a few days after the vaccine. Around half of people experience tiredness and a headache, and less than half have body aches, chills or feel feverish. These are all normal and expected side effects and are common with many other vaccines as well. They are signs that the immune system is learning how to recognize COVID.
For all these vaccines, these side effects will happen within a day or two of getting the vaccine and will disappear by the third or fourth day for most people. While there is a small chance that there will be a serious side effect, these are rare. Rare but serious side effects might be something like an allergic reaction. It’s always a great idea to speak with a health professional about any serious allergies or other health conditions or concerns you may have before you receive any vaccine.
Are vaccines developed with considerations given to how they might affect Black people different from other races?
Yes, around 10 per cent of the Pfizer and Moderna trial populations identified as Black. The studies demonstrated that there were no differences in efficacy or safety in any racialized or ethnic group. It is also important to note that there is no known evidence that would suggest that vaccines affect people differently based on racial differences. In the past, Black and Indigenous communities were used to test vaccines in what has widely been criticized and categorized as unethical today. The Moderna vaccine was co-developed by a Black immunologist named Dr. Kizzmekia Corbett.
Is the wait-and-see approach adopted by some members of the Black community before receiving their first dose putting them at greater risk?
Yes, vaccination is the best protection against severe disease arising from COVID-19 infection. Systemic racism means Black communities are more likely to live in crowded housing conditions or to work in higher-risk environments. When some members of the Black community decide “to wait and see” it can further increase the risk of COVID within the community. Often, people use a “wait and see” approach when they have certain questions or concerns about the vaccines. A better approach would be to discuss those concerns with a trusted health care provider or community leader. It’s important to note that the wait and see approach could have a similar risk for any racial or ethnic group depending on their risk of exposure. The lockdowns are effective measures, but they go against the vision of regional blocs of cooperating states—including the East African Community—free movement of everything from people to goods and resources. Instead, borders have been unilaterally closed, and the rapid retreat from regional cooperation has been the first refuge of the pandemic. While the health emergency indeed calls for lockdowns, border closures should have been part of regionally agreed strategies. But member states across the blocks called for cancelation of regional meetings and closure of boarders almost without any regional-level consultations. Indeed, most recently, Uganda has returned confirmed cases of truck drivers from Kenya and Tanzania to their countries after initially not including them in the national count of positive cases. Wouldn’t finding treatment where one tests positive signal greater regional integration?
If there is one lesson from the COVID-19 pandemic for Africa, it's the need to develop modern health care systems for all within national boundaries
The virus has also spurred politicians and government strategists to start thinking about more self-sufficiency, albeit in almost everything, from medical care to capacity to manufacture masks, hand sanitizers. When the storm passes, that thinking could extend to other fields, going against the economic sense of countries concentrating on comparative advantages while leveraging regional cooperation and supply chains for other needs. Indeed, if there is one lesson from the COVID-19 pandemic for Africa, it's the need to develop modern health care systems for all within national boundaries. The pace of transmission and the death toll of the virus has chilled the world and led to reckonings across Africa, as border closures and flight suspensions have meant that powerful and wealthy citizens have suddenly not been able to fly out for medical procedures at high-end hospitals outside their country.
The lockdowns are effective measures, but they go against the vision of regional blocs of cooperating states—including the East African Community—free movement of everything from people to goods and resources. Instead, borders have been unilaterally closed, and the rapid retreat from regional cooperation has been the first refuge of the pandemic. While the health emergency indeed calls for lockdowns, border closures should have been part of regionally agreed strategies. But member states across the blocks called for cancelation of regional meetings and closure of boarders almost without any regional-level consultations. Indeed, most recently, Uganda has returned confirmed cases of truck drivers from Kenya and Tanzania to their countries after initially not including them in the national count of positive cases. Wouldn’t finding treatment where one tests positive signal greater regional integration?
If there is one lesson from the COVID-19 pandemic for Africa, it's the need to develop modern health care systems for all within national boundaries
The virus has also spurred politicians and government strategists to start thinking about more self-sufficiency, albeit in almost everything, from medical care to capacity to manufacture masks, hand sanitizers. When the storm passes, that thinking could extend to other fields, going against the economic sense of countries concentrating on comparative advantages while leveraging regional cooperation and supply chains for other needs. Indeed, if there is one lesson from the COVID-19 pandemic for Africa, it's the need to develop modern health care systems for all within national boundaries. The pace of transmission and the death toll of the virus has chilled the world and led to reckonings across Africa, as border closures and flight suspensions have meant that powerful and wealthy citizens have suddenly not been able to fly out for medical procedures at high-end hospitals outside their country.
 The only thing that has preserved a certain level of regional importance are the multilateral financial institutions such as the
The only thing that has preserved a certain level of regional importance are the multilateral financial institutions such as the  There is little faith in how effective social distancing measures will be in slowing transmission for African cities from Lagos, Nigeria to Kampala, Uganda to Soweto Township in Johannesburg, South Africa—all of which have crowded informal settlements. The lockdowns are challenging given that a big part of the population in sub-Saharan Africa has no savings and lives hand-to-mouth daily.
Indiscriminate infections should be a reminder that all humans are equal, but they often only reveal the cruel, glaring social inequality in the world
The UN has called for emergency help for poor countries, and while that’s desired, it still carries a north-to-south dependency tone and could add to disentanglement sentiments in the COVID-19 pandemic's aftermath. That notwithstanding, African countries have taken the social distancing message to heart, they can’t afford to gamble with experiments like the U.K.’s herd immunity. Uganda, for example, shut down schools and places of worship even before confirming a single COVID-19 case. Is it time for us to reflect on what matters for humanity—perhaps taking lessons from princess Sofia who has temporarily set aside her tiara to work as a medical assistant in support of the fight against COVID-19 in Sweden?
There is little faith in how effective social distancing measures will be in slowing transmission for African cities from Lagos, Nigeria to Kampala, Uganda to Soweto Township in Johannesburg, South Africa—all of which have crowded informal settlements. The lockdowns are challenging given that a big part of the population in sub-Saharan Africa has no savings and lives hand-to-mouth daily.
Indiscriminate infections should be a reminder that all humans are equal, but they often only reveal the cruel, glaring social inequality in the world
The UN has called for emergency help for poor countries, and while that’s desired, it still carries a north-to-south dependency tone and could add to disentanglement sentiments in the COVID-19 pandemic's aftermath. That notwithstanding, African countries have taken the social distancing message to heart, they can’t afford to gamble with experiments like the U.K.’s herd immunity. Uganda, for example, shut down schools and places of worship even before confirming a single COVID-19 case. Is it time for us to reflect on what matters for humanity—perhaps taking lessons from princess Sofia who has temporarily set aside her tiara to work as a medical assistant in support of the fight against COVID-19 in Sweden?
 How should we use available resources to bridge the inequality gap? These are the questions we should be asking. Yes, COVID-19 has divided us and it will challenge unions, but the baby shouldn’t be thrown out with the bath water.
How should we use available resources to bridge the inequality gap? These are the questions we should be asking. Yes, COVID-19 has divided us and it will challenge unions, but the baby shouldn’t be thrown out with the bath water.